How a droopy eyelid is evaluated — margin reflex distance, levator function, the phenylephrine (Neo-Synephrine) test, Hering's law, and visual-field impact.
Medically reviewed by Steven Leibowitz, MD·Oculoplastic Surgeon·Last updated June 2026
Part of our complete guide to Ptosis (Droopy Eyelid) — this page covers ptosis evaluation and diagnosis in depth.
Evaluation of Ptosis
Careful measurement is the foundation of ptosis surgery planning. Dr. Leibowitz records the following at every ptosis evaluation:
Video: What a Ptosis Evaluation Looks Like
Margin-reflex distance (MRD-1): the distance from the corneal light reflex to the upper lid margin in primary gaze. Normal ≈ 4–5 mm; ptosis is present when MRD-1 is < 2 mm
Levator function: total lid excursion from full downgaze to full upgaze with the brow held still. Excellent ≥ 10 mm; fair 5–9 mm; poor ≤ 4 mm — this single measurement largely determines the surgical approach
Lid crease height: the distance from the lash margin to the skin crease, which guides the incision level
Phenylephrine test: a drop of 2.5% phenylephrine behind the upper lid stimulates Müller’s muscle; elevation of ≥ 1 mm predicts a favorable response to internal ptosis repair (MMCR)
Hering’s Law of Equal Innervation
When ptosis affects only one eye — or is much worse on one side — Hering’s law becomes critical to surgical planning. Both levators receive equal central drive from the brain. In unilateral ptosis, the brain increases drive to both sides to keep the ptotic lid open. If surgery elevates the ptotic lid, that extra drive drops — and the fellow lid may fall.
This “see-saw” effect means apparent unilateral ptosis can unmask bilateral ptosis after surgery on one side. The interactive animation below demonstrates this phenomenon.
PtosisHering's Law Visualization
Slide the control to see how ptosis in one eye affects the fellow eye according to Hering's Law of Equal Innervation.
Pre OperationPost Operation
Drag the slider to compare
The Phenylephrine (Neo-Synephrine) Test
2.5% Phenylephrine (Neo-Synephrine) Response
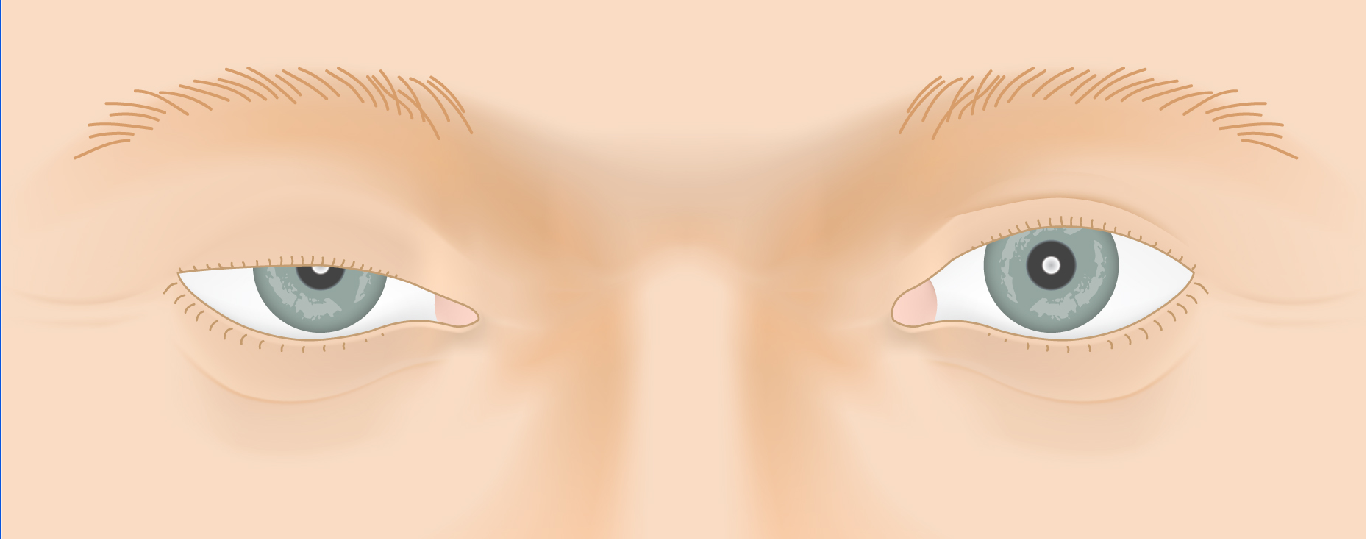
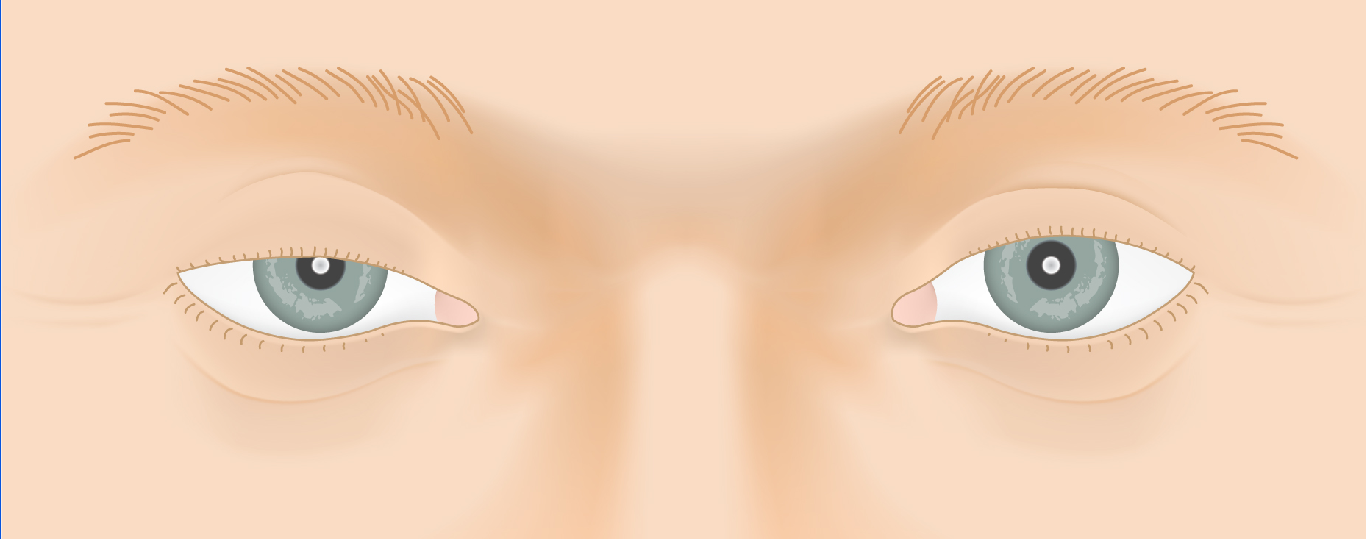
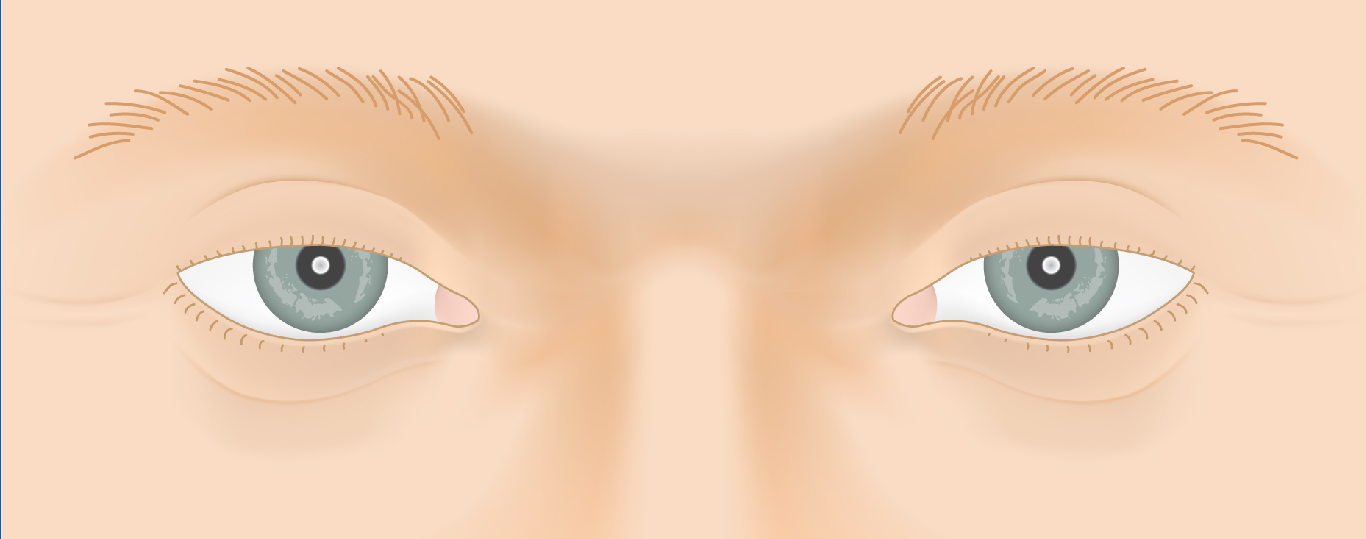
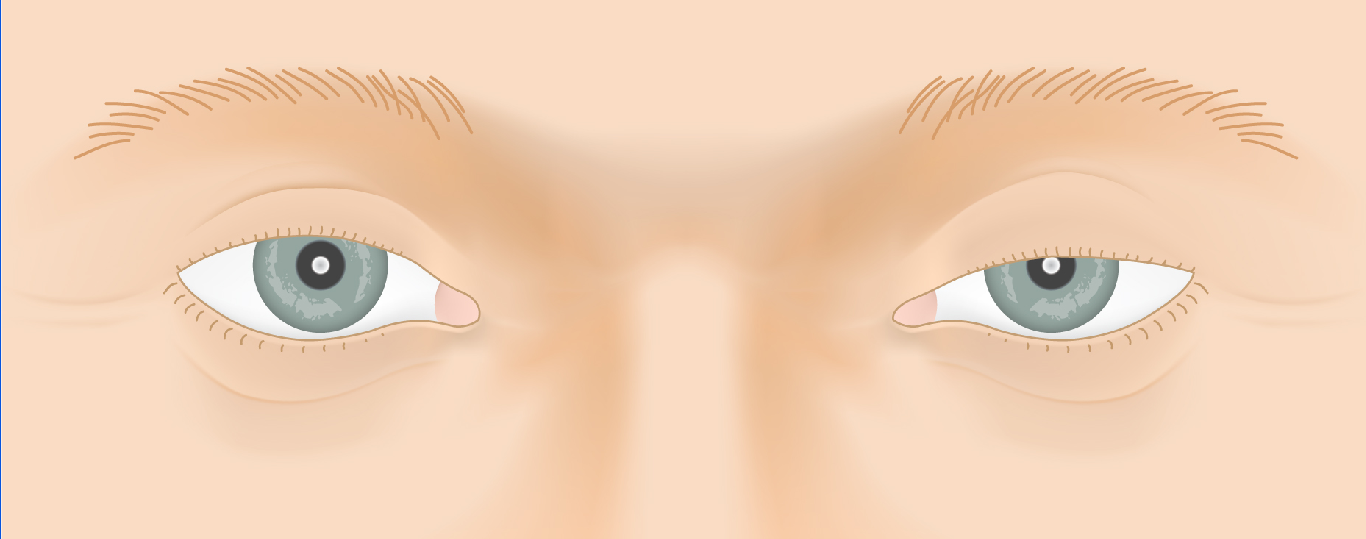
Four candidates evaluated for an internal (Müller's-muscle) repair — step through each before and after the drop.
BeforeAfter
⟺
Drag the divider to compare each candidate before and after the 2.5% phenylephrine (Neo-Synephrine) drop — a lid that lifts predicts a good response to internal (Müller's-muscle) repair.
Instilling 2.5% phenylephrine (Neo-Synephrine) drops stimulates Müller’s muscle. If the eyelid then lifts to a good height, the patient is an excellent candidate for an internal (Müller’s muscle–conjunctival resection) repair. This quick in-office test directly guides the choice of operation.
Key Measurements
Margin reflex distance (MRD-1): the distance from the corneal light reflex to the upper-lid margin (normal ~4–5 mm); a reduced MRD-1 quantifies the ptosis.
Levator function: upper-lid excursion from down-gaze to up-gaze (good ≥ 10 mm; fair 5–9 mm; poor ≤ 4 mm) — the single most important measurement for selecting the operation.
Palpebral fissure height and lid-crease position: a high or absent upper-lid crease points to aponeurotic dehiscence.
Ptosis vs. Blepharoplasty
Two distinct upper eyelid conditions are often confused. Understanding the difference determines which operation is appropriate — and whether insurance will cover it.
Ptosis
Drooping of the eyelid margin itself
Eyelid margin sits too low across the pupil
Caused by weak or detached levator / Müller’s muscle
Little or no excess skin
Surgery elevates the eyelid margin
May be covered by insurance with visual field documentation
Dermatochalasis (Pseudoptosis)
Excess skin overhanging the lid
Eyelid margin sits at normal height
Overhanging skin hood blocks the superior field
Repaired by blepharoplasty (skin removal)
Can coexist with true ptosis
May be insurance-covered when the skin demonstrably obstructs the superior visual field
Ptosis — the lid margin sits lowDermatochalasis — excess skin, normal margin
Both conditions can be present simultaneously. Ptosis repair and blepharoplasty are frequently combined in a single operation through the same eyelid crease incision.
Chiefly by the margin reflex distance (MRD-1) — how far the upper lid sits from the corneal light reflex — and by levator function, the lid's up-and-down excursion. Together these grade the ptosis and select the operation.
What is the phenylephrine (Neo-Synephrine) test for?
Drops of 2.5% phenylephrine stimulate Müller's muscle; if the lid lifts well, an internal (Müller's muscle–conjunctival resection) repair is likely to work — so the test helps choose the approach.
Why does one eyelid look droopier after the other is lifted?
Hering's law of equal innervation — both lids receive equal lift signals. When a ptotic lid is doing extra work, the fellow lid can look high; correcting one side may unmask droop on the other, which the evaluation anticipates.
Your Surgeon
Steven Leibowitz, MD
Cosmetic and Reconstructive Surgery of Eyelids, Orbits, and Tear Ducts